Beverly Cosgrove, 2/15/2023, Version 23
What’s wrong with Spironolactone? Lots.
Spironolactone (“Spiro”) is a potassium-sparing diuretic and steroid drug frequently prescribed in the US to assigned-male-at-birth (AMAB) trans women as part of their HRT. However, the drug has a number of mild to severe mental side effects, can lead to bodily changes which most trans women might consider disfiguring, and may interfere with breast development and other feminization.
Spiro began being prescribed to trans women in the early 90’s, when the dangers of taking estrogens in the form of Ethinyl Estradiol or Premarin became known. The use of Estradiol alone, without any kind of antiandrogen, is well known to be capable of suppressing testosterone to female levels. (Refs 2,3,4,5) However in the 90’s, the Estrogen-related dangers were known to be proportional to dose, and several studies demonstrated an elevated risk of cardiovascular disease within the first 1-2 years of HRT initiation. (Ref 6) Studies at the time unfairly lumped all estrogens together, and all progestins together, as having the same dangers, a mistake which still lingers today. (7) As a result of their unwillingness to treat trans women with high levels of estrogen, Spiro was added to many HRT regimens in the US to assist in suppressing testosterone levels and blocking testosterone effects. Its use has persisted despite the availability of safe and effective human-identical estradiol.
Spironolactone does NOT feminize significantly, though it is known to encourage some gynecomastia in males. Its sole use in trans patients is to reduce the effect of testosterone, and also testosterone levels, a job that estradiol would do if a suitable estradiol-only regimen were used instead. Today, AMAB transsexuals often begin their HRT in the US with an “orthodox protocol” consisting of 2-4mg a day of estradiol in pill form plus 200mg a day of Spironolactone. Physicians favor this approach because it gives a fairly quick reduction in erectile capability which can give some fast relief to genitally dysphoric transsexuals.
But there are problems associated with Spiro that your doctor may not tell you about.
Spiro makes it more difficult for patients to reach a normal female hormone balance. There are two effects, (1) Inability to achieve female level testosterone, and (2) resistance to normal utilization of estradiol. These two effects happen concurrently.
The first effect is that Spiro doesn’t work well in reducing testosterone. A long term study of New York clinic patients showed that Spiro was unhelpful in achieving basic HRT goals. “We unexpectedly did not find that Spironolactone aided in testosterone suppression and further found that it seemed to impair the ability to reach desired serum 17-β estradiol levels.” (26) and “Spironolactone did not enhance testosterone suppression, and finasteride was associated with higher testosterone levels.” (28) In another recent study of patients following a Spironolactone and estradiol protocol, followed for as long as 3.5 years showed that the majority did not attain female levels of testosterone in the first couple of years, with only about half attaining it by year 3. “Patients with normal BMI started with the highest level of testosterone and demonstrated the steepest decline between initial visit and 9 months but seemed unable to achieve levels of testosterone in the female physiological range overall.” Obese patients whose testosterone was already lower than average had somewhat better success with lowering testosterone, but results were still poor. (23) In the chart below, taken from the same study, the yellow band shows the female normal testosterone level. Only after 3 years of treatment did at least half of patients fall into that band. Compare this to the profound drop in testosterone caused by even a single injection of estradiol, in as little as 36 hours. “Suppression of plasma testosterone levels from a mean of 760 ng/dl… in normal young adult men… to 123 ng/dl was noted 36 h after estradiol administration.”(2) In this sense, a single estradiol injection accomplishes what the Spiro-based protocol may need over 3 years to do. 
The second effect: taking Spiro, for reasons that are not well understood, appears to interfere with the patient achieving expected blood levels of estradiol. In a recent study, patients taking Spiro were found to be unable to achieve expected estradiol levels. “Estradiol levels of patients did not correspond with estradiol dosage administered or BMI. There was no discernable change in serum estradiol levels despite the fact that patients commenced and then continued to take what was believed to be supra-physiologic exogenous estradiol.” (23) and “Spironolactone, but not finasteride, use was associated with impairment of obtaining desired 17-β estradiol levels.” (28)
Spironolactone causes patient cortisol levels to rise. (Ref 1) Patients taking Spiro at doses as low as 25mg a day experience significantly elevated cortisol levels within a few weeks. (8) However, typical dose for trans women is 200mg per day, despite it being known that doses over 100mg have diminished effect. (9) Normally, the circulating levels of cortisol are tightly controlled by the hypothalamic-pituitary-adrenal (HPA) axis. A key feature of the HPA axis is negative feedback regulation, whereby cortisol suppresses its own secretion. Spiro activates the HPA axis. However, chronic activation of the HPA axis may play a pathogenic role in a wide range of common metabolic and psychiatric disorders, including obesity, depression, and age-associated cognitive dysfunction. (1) In particular, depression which does not respond to common anti-depressant therapy has been noted in patients with hypercortisolism due to disruption of the HPA axis, which generally resolves itself once the cause is removed. (16,18)
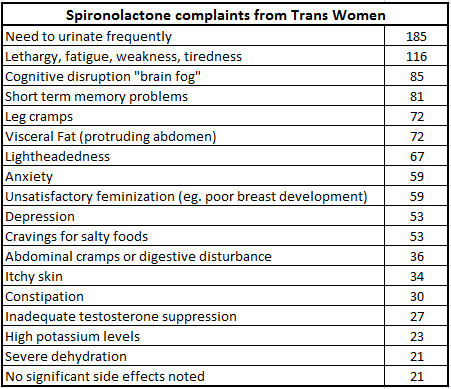 The effects of Spiro on the brain’s mineralocorticord system are complex. The primary result as cortisol is raised is a crippling of certain thinking processes, selective attention, visuospatial memory, and mental flexibility/set shifting. There is also a modulation, both up and down, of panic and anxiety and ability to withstand stress. (10) Considering that the time of beginning of a transsexual’s hormonal transition may be one of the most stress-inducing periods of the person’s life, it is not surprising that patients receiving Spironolactone complain of “brain fog”, poor memory, irritation, anxiety and panic attacks. This also begs the question: could the start of Spiro-based HRT also explain increased incidence in the transgender community of self harm, addictive behavior, and suicide? Data to answer this question is lacking, but the risk seems rational and clear, and this complex of issues — brain fog, poor memory, lethargy, depression, anxiety and panic attack — are widely known in the transgender community. (11) [and Chart (15)] Especially worrying is the evidence that, if a patient is already depressed, adding Spironolactone greatly accelerates the level of hypercortisolism it induces, creating feedback which traps the individual in a depressive state which does not respond to antidepressants. (18)
The effects of Spiro on the brain’s mineralocorticord system are complex. The primary result as cortisol is raised is a crippling of certain thinking processes, selective attention, visuospatial memory, and mental flexibility/set shifting. There is also a modulation, both up and down, of panic and anxiety and ability to withstand stress. (10) Considering that the time of beginning of a transsexual’s hormonal transition may be one of the most stress-inducing periods of the person’s life, it is not surprising that patients receiving Spironolactone complain of “brain fog”, poor memory, irritation, anxiety and panic attacks. This also begs the question: could the start of Spiro-based HRT also explain increased incidence in the transgender community of self harm, addictive behavior, and suicide? Data to answer this question is lacking, but the risk seems rational and clear, and this complex of issues — brain fog, poor memory, lethargy, depression, anxiety and panic attack — are widely known in the transgender community. (11) [and Chart (15)] Especially worrying is the evidence that, if a patient is already depressed, adding Spironolactone greatly accelerates the level of hypercortisolism it induces, creating feedback which traps the individual in a depressive state which does not respond to antidepressants. (18)
But Spiro can actually sabotage the very physical changes that trans women seek through HRT. Increased cortisol is associated with accumulation of visceral fat — hard fatty deposits interlaced with internal organs which causes a swollen belly. It is important to discriminate between belly adipose fat, which is soft “jelly like” fat directly under the skin, and visceral fat which is behind the abdominal wall. Visceral fat requires significant effort with diet or exercise to remove and cannot be removed with any kind of ordinary plastic surgery. (20) This visceral fat is caused by raised cortisol. The informal term “Spiro belly” arose because of the perception that those on high doses of Spiro for long term (200mg/day for over a year) seem to often have the characteristic protruding belly. Once visceral fat has accumulated, it is difficult to achieve an ideal waist-to-hip size ratio again, even if Spiro is stopped and diet and exercise is tried. Research on young girls with poor Waist/hip measurements correlate to higher cortisol levels and visceral fat, as well as mobilization of fat from elsewhere in the body to the central region — the opposite of the desired fat mobilization sought by trans women. (12) The association between hypercortisolism, major depressive illness, and deposits of visceral fat has been well established. (17)
Finally, Spiro use is associated with poor breast development in trans women. A preliminary study showed that patients using Spiro instead of another antiandrogen (such as Cyproterone) had significantly more dissatisfaction with breast development. (13) At this point, the causation is uncertain. The cause could be the known tendency for Spiro to interfere with the blood levels of estradiol, as verified in multiple studies (23,28). However, it is also known that elevated cortisol suppresses Human Growth Hormone, resulting in smaller stature (14) and therefore possibly, reduced breast growth even in later life. Regardless of the exact explanation, if appears that Trans women are doubly penalized for Spiro use in this respect, because chest measurement to waist measurement ratio may be sabotaged at BOTH ends – the very opposite of an “hourglass figure”.
If you are taking Spironolactone now, and wish to quit, please be warned — quitting Spiro suddenly without preparation is difficult and hazardous, and your doctor is very unlikely to understand some of the problems you will encounter. You should be able to find some peer coaching on the practical aspects of quitting in the Facebook HRT group for more information. Also, experience suggests that most trans women on megadoses of Spiro (200mg or higher) can successfully suddenly drop to 100mg a day without rebound effects (speak to your doctor), but following that, a slower reduction schedule may be required. But the best solution regarding Spiro is to never start.
Medical specialists and providers have seen the evidence and are finally reconsidering Spiro. A leading Transgender hormone specialist, Dr. Will Powers, has become outspoken in his opposition to the orthodox low-estrogen high-Spiro legacy/orthodox treatment protocol. (27) With over 1000 patients in his practice, Dr. Powers has established avoidance of antiandrogens, especially Spiro, as a key to his “Powers Method”. Another key provider with a somewhat similar approach is Dr. Kristen Vierregger. Both these doctors were an influence on, and were probably indirectly influenced by, this very article you are reading since its first version in 2014.
 Permit me to digress a little here with some commentary. Spironolactone was made part of HRT based on standards set by The Endocrine Society (19,21) among others. By setting a standard for estradiol levels based on 90’s-era risk data about Premarin and Provera, the most dangerous forms of HRT, and ignoring the risk reduction of estradiol 17b given parenterally, they created an artificial standard based on what they did not know rather than what they did know. But we know much more now. The risks of injected estradiol levels in the 300-500 pg/ml range are far lower than the risks of suicide or psychotic episodes or sustained mental illness due to mood disturbances from the antiandrogens the prescribers are now offering their patients to keep them below that level. The prescribers are saving their patients from a small risk by exposing them to a larger risk. It is bad risk-benefit judgement. I have written more on this elsewhere. (7) It is notable that the 2009 version of The Endocrine Society guidelines even include a mention of estradiol injection (19) but still refer to Spironolactone. One final thought, this time a speculation: it seems possible based on observations that high levels of testosterone provide some protection against the cortisol-raising properties of Spironolactone, such that testing of the drug on male volunteers might not have shown such a large side effect when the drug was originally tested, leading to a situation where heavy dosing of trans women led to these oversized effects. Would the original manufacturer’s dosing advice have been different if the drug had been more thoroughly tested with female patients? Something worth looking into, perhaps.
Permit me to digress a little here with some commentary. Spironolactone was made part of HRT based on standards set by The Endocrine Society (19,21) among others. By setting a standard for estradiol levels based on 90’s-era risk data about Premarin and Provera, the most dangerous forms of HRT, and ignoring the risk reduction of estradiol 17b given parenterally, they created an artificial standard based on what they did not know rather than what they did know. But we know much more now. The risks of injected estradiol levels in the 300-500 pg/ml range are far lower than the risks of suicide or psychotic episodes or sustained mental illness due to mood disturbances from the antiandrogens the prescribers are now offering their patients to keep them below that level. The prescribers are saving their patients from a small risk by exposing them to a larger risk. It is bad risk-benefit judgement. I have written more on this elsewhere. (7) It is notable that the 2009 version of The Endocrine Society guidelines even include a mention of estradiol injection (19) but still refer to Spironolactone. One final thought, this time a speculation: it seems possible based on observations that high levels of testosterone provide some protection against the cortisol-raising properties of Spironolactone, such that testing of the drug on male volunteers might not have shown such a large side effect when the drug was originally tested, leading to a situation where heavy dosing of trans women led to these oversized effects. Would the original manufacturer’s dosing advice have been different if the drug had been more thoroughly tested with female patients? Something worth looking into, perhaps.
The TransFemScience site has responded to points made in this article regarding visceral fat with a detailed rebuttal. It is well worth reading. It states in part, “The influence of spironolactone on cortisol levels in clinical studies is variable and the magnitude of effect is limited. Hence, the clinical significance of increased cortisol levels with spironolactone is uncertain.” And also points out, correctly, that detailed studies have not been done which support our visceral fat suspicions. Even though Spiro use is known to be associated with raised cortisol levels, and even though high cortisol is proven to be capable of causing visceral fat, the TFS site is suggesting that “the dots are not connected” in the way I have proposed. I continue to assert that Spiro use can lead, in some cases, to accumulations of visceral fat. Studies are cited at the TFS site, but note that the data is largely for low dose Spiro. Our observation is that these effects do not begin until the patient is taking doses of 100-400 mg a day, and takes these doses for at least 12 months. Transgender women are being exposed to doses which far exceed the studied levels being used to claim safety. Our own observations seem to indicate that taking less than 100mg daily, or taking Spiro for 12 months or shorter time usually does NOT lead to visceral fat accumulation. We are raising the red flag on a patient population exposed to a MUCH greater dose. Finally, there is the inevitable labeling of our observations as “anecdotal evidence” (or even drug-blaming from patients unhappy about unrelated issues). Let me just point out that much important medical knowledge starts out as anecdotal. Collect a large group together, and those anecdotes become “group knowledge”, which can progress to shared beliefs and practices, and then to clinical experience, and from there it may become accepted into the bulk of accepted medical science. New knowledge always starts somewhere.
The medical community owes it to the transsexual community to take a second look at the overall risk/benefit ratio for the use of Spironolactone as an antiandrogen. Not only is there evidence that Spiro may be interfering with the primary goal of HRT, but Spiro may be directly responsible for patient harm by crippling the cognitive ability of patients and compromising their ability to withstand stress — a terrible burden for this highly stressed minority.
SOME ANECDOTAL EXPERIENCES
—
“The short term memory deficit and cognitive impairment were debilitating side effects of 25mg over a month’s time. This along with unusual bruising,dizziness/unsteadiness, and chronic exhaustion prompted me to stop taking it. I can’t imagine what might have happened with the common higher doses.”, MT, December 2016
—
“Was on that crap for 21 months. Lowered it from 200mg/day to 100, then 50, then 0. This was in Oct. of this year. Since then all the symptoms are going away. I also stopped using finasteride. Switched from pills and oral P4 to injectable EV and P4. 5mg EV and 20mg P4 every 3.5 days. Feeling much better.”, KA, Dec 2016.
—
“After taking it for about 4 years it started to just quit blocking T all together. I was on injected estradiol valerate and yet my T was at 400! Believe me that Spiro is bad shit. It cost me my job. The brain fog and short term memory loss may be permanent. Depression was increased and not to mention the long term memory I lost.”, SL, Dec 2016.
—
“I had a lot of emotive/cognitive issues with Spiro that noticeably improved when I dropped it after two years (my high E2 level allowed this).” BRB, Dec 2016.
—
“I had a bout of severe dizziness and got a very itchy rash which my housemates initially thought was a bug bite then later confirmed it was not like any bug bite they’d ever seen. The rash grew larger and more itchy over the course of a week, it disappeared completely a day or two after I stopped taking Spiro. While on Spiro I experienced greater difficulty with organizing thought, more frequent thought derailment, and more reactionary and unclear thinking. These severely impacted my job performance as I rely heavily on memorized diagnostic procedures to solve computer problems. The mental side effects of Spiro dissipated quickly for me after I stopped taking it.”, RM, Dec 2016.
—
“I personally can’t stand Spiro! Been on it since May…tomorrow is 7 months. I’ve had severe side effects since the beginning. Here is my list: tired, memory loss, brain fog, light headed, anxiety, poor breast development, severe depression, constipation, dehydration, and low blood pressure. I’ve been a mess since the beginning. I take the pill form. Looking into asking my doctor about moving over to injections and switching to progesterone and keeping my estradiol going.”, JMS, Dec 2016.
—
“I was on it for 6 months at a low dose, stopped taking and upped my. Estridol and progesterone. I don’t and didn’t want to start down the road. Had the mental side effects.”, DBS, Dec 2016.
—
“my endo started me on 200mg spiro daily with estradiol and i started getting spells of difficulty breathing, debilitating migraines (which i have never experienced before/not a headachey person), increased anxiety, fatigue, yadda yadda. she really didnt think it was the spiro (and theres not too much info about spiro online??) but we cut it out and i cant begin to tell you how much better i feel” DS, 1-5-18
—
“Started on Estradiol and Spiro pills… Wasn’t getting anywhere with my E and T levels. After 6 months, switched to EV injections and dropped the Spiro, because of this forum. Now I’m consistently in ideal range of E and T. It’s very possible with no Spiro.”, AA, 1-5-18
—
“I switched from spiro to cypro only a few days ago. Ok, its still an AA, but its the lesser of two evils as Beverly pointed out in a previous thread when I asked. In that few days, the brain fog has already gone, I have elevated energy levels and i’m not feeling tired constantly. I no longer pee like a race horse. Getting off spiro will only benefit your health. If my E levels are right next week when I go for my bloods, i’ll be dropping the cypro too.” EC, 1-5-18
—
“I have a bad reaction to antiandrogens. I’m now completely off of spironolactone, feminizing rapidly, feel very healthy, and have no brain fog or other symptoms typical to longer term exposure to anti androgens. I’m just taking injectable estradiol valerate at a normal dosage, subcutaneous twice a week to keep levels more stable, and micronized progesterone. I am pre-op and my testosterone is actually lower than the female index range without antiandrogens.”, JM, 1-6-2017
—
“I dropped 200mg of daily Spiro. Increased my E from 4mg to 8mg. My E increased and T dropped and got my libido back. Worked for me. In two weeks at next DR. appt, I am going to ask to switch from pills to injections.”, SK, 8-1-2018.
—
“I too feel 1000 times better since dropping Spiro and taking no AAs, I like the E and p only for T suppression, works way better that I had ever expected, almost too good actually.”, RS, 1-8-2018.
—
“I was only on it about 1.5 months and already had bad brain fog and possibly other developing issues. I THINK am in the clear for any permanent negative effects from it, but I worry.”, NK, 6-1-2020.
—
“I hate Spiro and only took it for a couple of months. It caused sharp pains in my muscles, and also caused deep depression. I will never take it again. There are several alternatives to Spiro. Another I will not take is Finasteride, due to it’s side effects.”, AT, 5-27-2020.
—
“I was on both low E doses and high spiro. Thought I was done with my programming career. Now I’m on EV, progesterone and no blockers. My brain is back.” K.L., 4-30-2021
—
“I’m a lot better since dumping spiro. I started to calm down upon starting E, but brain fog got worse – not to mention I was constantly dehydrated. Estrogen – WITHOUT spiro – has vastly improved the cognitive issues I had in the 10 years prior to HRT, killed the rhoid rages, and continues to heal the depression and other emotional issues I had had since starting puberty.”, J.D., 4-30-2021
REFERENCES and LINKS
(1) “Combined Receptor Antagonist Stimulation of the Hypothalamic-Pituitary-Adrenal Axis Test Identifies Impaired Negative Feedback Sensitivity to Cortisol in Obese Men”, Mattsson C, The Journal of Clinical Endocrinology & Metabolism, Volume 94, Issue 4, 1 April 2009, Pages 1347–1352, https://doi.org/10.1210/jc.2008-2054
(2) “ Direct inhibition of Leydig cell function by estradiol.”, Jones TM, J Clin Endocrinol Metab. 1978 Dec;47(6):1368-73.
(3) “ The effect of oestrogen administration on plasma testosterone, FSH and LH levels in patients with Klinefelter’s syndrome and normal men.” Smals AG, Acta Endocrinol (Copenh). 1974 Dec;77(4):765-83.
(4) “In men, peripheral estradiol levels directly reflect the action of estrogens at the hypothalamo-pituitary level to inhibit gonadotropin secretion.”, Raven G, J Clin Endocrinol Metab. 2006 Sep;91(9):3324-8. Epub 2006 Jun 20.
(5) “Sex steroid control of gonadotropin secretion in the human male. II. Effects of estradiol administration in normal and gonadotropin-releasing hormone-deficient men.”, Finkelstein JS, J Clin Endocrinol Metab. 1991 Sep;73(3):621-8.
(6) “Hormone Therapy Dose, Formulation, Route of Delivery, and Risk of Cardiovascular Events in Women: Findings from the WHI Observational Study”, Shufelt C, Menopause. 2014 Mar; 21(3): 260–266.
(7) “What Went Wrong With MTF Hormonal Therapy?“, Cosgrove, B.
(8) “Effect of eplerenone versus spironolactone on cortisol and hemoglobin A₁(c) levels in patients with chronic heart failure”, Yamaji M, Am Heart J. 2010 Nov;160(5):915-21
(9) “Spironolactone Dose-Response Relationships in Healthy Subjects”, McInness G, Br. J. clin. Pharmac. (1982), 13, 513-518
(10) “Blockade of the Mineralocorticoid Receptor in Healthy Men: Effects on Experimentally Induced Panic Symptoms, Stress Hormones, and Cognition”, Otte C, Neuropsychopharmacology (2007) 32, 232–238
(11) “Hormone Therapy is Lifesaving — But Why is No One Studying Its Long-Term Effects?“, Out Magazine, Tourjee D, 2016-09-20 09:38
(12) “Stress and Abdominal Fat: Preliminary Evidence of Moderation by the Cortisol Awakening Response in Hispanic Peripubertal Girls”, Donoho C, Obesity (2011) 19, 946–952
(13) “Predictive Markers for Mammoplasty and a Comparison of Side Effect Profiles in Transwomen Taking Various Hormonal Regimens”, Seal LJ, The Journal of Clinical Endocrinology & Metabolism, Volume 97, Issue 12, 1 December 2012, Pages 4422–4428
(14) “Cortisol and growth hormone: clinical implications of a complex, dynamic relationship”, Stratakis CA, Pediatr Endocrinol Rev. 2006 Apr;3 Suppl 2:333-8.
(15) Chart from active survey of over 200 Spironolactone patients, from Online Facebook Group, “The MTF Trans HRT Hormone Forum“, founded Dec. 2014, membership approx 9800.
(16) “Handbook of Stress and the Brain: Stress: integrative and clinical aspects”, Elsevier. pp. 440–
(17) “Increased Intra-Abdominal Fat Deposition in Patients with Major Depressive Illness as Measured by Computed Tomography”, Thakore J, BIOL PSYCHIATRY 1997;41:1140-1142
(18) “Mineralocorticoid receptor function in major depression”, Young EA, Arch Gen Psychiatry. 2003 Jan;60(1):24-8.
(19) “Endocrine Treatment of Transsexual Persons:An Endocrine Society Clinical Practice Guideline”, Hembree W, The Journal of Clinical Endocrinology & Metabolism, Volume 94, Issue 9, 1 September 2009, Pages 3132–3154
(20) “High visceral fat mass and high liver fat are associated with resistance to lifestyle intervention.”, Thamer C, Obesity (Silver Spring). 2007 Feb;15(2):531-8.
(21) “Endocrine Treatment of Gender-Dysphoric/Gender-Incongruent Persons: An Endocrine Society Clinical Practice Guideline”, Hembree WC, The Journal of Clinical Endocrinology & Metabolism, Volume 102, Issue 11, 1 November 2017, Pages 3869–3903
(22) “The 45-year story of the development of an anti-aldosterone
more specific than spironolactone”, Menard J, Molecular and Cellular Endocrinology 217 (2004) 45–52
(23) “Testosterone Levels Achieved by Medically Treated Transgender Women in a United States Endocrinology Clinic Cohort”, Liang J, Endocrine Practice: February 2018, Vol. 24, No. 2, pp. 135-142.
(24) “The effect of oestrogen administration on plasma testosterone, FSH and LH levels in patients with Klinefelter’s syndrome and normal men.” Smals AG, Acta Endocrinol (Copenh). 1974 Dec;77(4):765-83.
(26) “Hormonal Treatment of Transgender Women with Oral Estradiol“, Leinung M., https://doi.org/10.1089/trgh.2017.0035
(27) Dr. Will Powers, Video lecture, “Anti-Androgens and Spironolactone issues in MTF HRT | Dr Will Powers @ OUWB” Youtube link: https://youtu.be/LX8AdkL7u0s
(28) Leinung M.C., Feustel P.J., Joseph J. Hormonal treatment of transgender women with oral estradiol. Transgend. Health. 2018;3:74–81. doi: 10.1089/trgh.2017.0035.[PubMed]

I been on and still on the Spironolactone 200 mg. a day. I been on the 0.1 mg. Estradiol, 3 patches a week about 33 months. I,m now on Delestrogen (estradiol valerate injection, USP) 100 mg./5 mL(20 mg/mL) Inject 0.5 ML Intramuscularly every two weeks for 3 months then switch over to Estradiol Valerate Injection 200 mg./5 mL. Inject 0.5 MLS Intramuscularly Every Two Weeks for 3 months = total of 6 months supply. I am a 64 year old 01/05/1954 single mix breed Native American Pre/Op transgender women live alone over 40 years. My breast are not really big normal size, yet I stress out a lot not being fully developed, high cost of out of pocket cost $$$$ and what my retirement Health Ins.will pay. I was approved in full vaginoplasty and breast surgeries on my Employers Cobra Health Ins.$714.40 month premiums. My Cardiology Doctor said all surgeries are to be cancelled until I get a MRI scan done first. While waiting for my appointment MRI scan two months later my Social Security Medicare plan took over where I pay about with the Extra Help $135.00 monthly premiums. After I pass the Stress Test instead of MRI scan that I call my to Health Insurance about what they will and will not cover threw their plan? Their plan said I will have to pay out of pocket about $6,500.00 for vaginoplasty surgery, $350.00 for the first 5 days in recovery room in hospital and after that will be cover in full with no extra charge. The breast surgery will not be cover. I told from Social Service I make to much money on Social Security to get Medicaid. I work over 40 years of my single life paying into Social Security, Medicare, Fed. and State Taxes and not able to get Medicaid. I am able to get about $15.00 month on Food Stamps and notable to get Heep program to help pay some my heat bills.
LikeLike
Rhonda, the problem with your estradiol injection routine is the two week interval. You generally cannot get reliable testosterone suppression using a two week interval — if you inject by gluteus, a 7 day interval works for most. If you inject by thigh, you should not go more than 5 day interval. Success with estradiol by injection is more a matter of avoiding dropouts than in achieving high peaks. The two week interval is probably the most common mistake made by prescribing doctors — that interval only works for women with productive ovaries. Even if you are a trans woman without testicular tissue, 14 days is too long, and may contribute to stress an depression. Doctors are usually amenable to you injecting half doses twice as often.
LikeLike
Thank you for writing this article! I am a 36 y/o trans woman who plans on starting HRT this year. My latest blood test showed a T level of 264. If I can successfully convince my endo to not force spiro on me, I’d rather not take it. Is it possible to only take E off the bat and avoid AAs altogether from the start? And in your opinion, should I try to get him to prescribe IM EV right away? I know a lot of docs and endos seem to prefer to prescribe sublingual E for months at first. I’ve heard it can be challenging to convince endos to think outside their normal box, and I live in a smaller city without a PP or many options at all for docs / endos willing to supervise HRT. But I’ve heard that IM is the most effective for a lot of folks, and I’d rather inject every 5-7 days than have to let pills dissolve slowly in my mouth 2-3 times a day. Anyway, thank you for any advice you can provide!
LikeLiked by 1 person
Jocelyn, it is widely known among patients that IM estradiol gives superior results compared to any kind of oral estradiol, and trying to get prescribers to recognize this fact is a common problem. Yes, generally if one begins with an injection regimen with no antiandrogen at all, the levels of testosterone begin a slow decline and in 1-6 months reaches female normal levels. See my other article https://transhormones.wordpress.com/2017/11/19/the-top-12-myths-about-injections-for-mtf-trans-people/
Good luck!
LikeLiked by 1 person
Hi ! Beverly ,
I am a transwoman in my 50’s now I started out I would say I was probably about 38 or so not quite 40 , I was on the estradiol only for years with no blockers at all and this was when I was self medicated , I was told I needed to be under a doctors care, which I did see a dr. eventually after self medicating . He put me on Spiro and E , cause I was adv that this would work better to achieve certain goals. Now as far as I know from taking Spiro I haven’t had any side effects as I am reading about here .
I had some female characteristics anyway at birth , taking the Est only did feminize me very well with a nice hour glass figure and nice skin , which I have a very nice complexion thank God,,
After all these horror stories even though at the moment I don’t have any issues with this as far as I know nothing to mention only that it has caused my hair to grow faster over the course of using Spiro.
INconclusion , I wanting to stop the spiro all together and just start on Estrogen only again as I use to , I mean through the years I have developed nicely , even with breasts development , so I can’t say that I have had any bad side effects.
LikeLike
[…] increase in self harm, suicide, and addictive behavior in this highly stressed patient population. (18) Also, antiandrogens have been shown to sabotage success in full feminization, fat mobilization, […]
LikeLiked by 1 person
[…] beginning HRT. The possibility that harm is being done to the patient cannot be dismissed. See my article on Spironolactone in […]
LikeLiked by 1 person
I was given 50 mg of spiro daily and .5 estridol once a week to start i think this isnt enough to get things going well
LikeLiked by 1 person
“Visceral fat cannot easily be reduced with diet or exercise and cannot be removed with any kind of plastic surgery. (20) ”
“Once visceral fat has accumulated, it is difficult or impossible to ever achieve an ideal waist-to-hip size ratio again, even if Spiro is stopped and diet and exercise is tried.”
These statements are blatantly wrong. Ten minutes of research is enough to figure out what you’re saying is genuinely not true. Visceral fat can absolutely be lost through weight loss.
What’s worse is that the paper you use (20, http://onlinelibrary.wiley.com/doi/10.1038/oby.2007.568/full ) to make these claim does not back up your statements. That paper discusses the success of lifestyle intervention (resulting in weight and fat loss) and its effectiveness on increasing insulin sensitivity. That paper you cited suggests that lifestyle intervention may have less effect on increasing insulin sensitivity for those who have higher BMI and visceral fat stores when starting lifestyle intervention compared to those who have lower BMI and visceral fat stores given the same amount of BMI/visceral fat loss. The paper does NOT make any claims about the ease with which visceral fat can be lost in comparison to adipose fat, nor does it remotely make any claims suggesting that an ideal waist-to-hip measurement ratio becomes “difficult or impossible to ever achieve.” The paper isn’t relevant to either of these claims.
Please, do actual research and find good sources before making extreme statements. You’re going to scare the hell out of trans women with blatantly wrong statements like that. I spent a long time looking and I have not found any research suggesting visceral fat gain is largely irreversible. Telling people that if they gain visceral fat they’ll never be able to lose it and they’ll never be able to change their hip/waist ratio afterwards is both irresponsible and incorrect. You should not be making such dangerous statements like that without a hell of a lot of material to directly back up your argument.
LikeLiked by 1 person
Good points, and I’ve incorporated them into the article. The emphasis is that visceral fat is caused by high cortisol levels (among other things) and requires dieting combined with a fairly substantial (though not extreme) exercise regimen to get significant improvement. It’s still a scary thing to get abdominal fat that’s difficult to remove, and certainly it is not the desired result of a trans woman’s HRT. And it is also of concern that unless and until it is removed, it is associated with risks of metabolic syndrome and insulin insensitivity. And it is truly difficult to remove, and requires a significant effort – if you are a sedentary person, your chances of getting rid of it are small to none.
LikeLiked by 2 people
No-carb diet is more effective for weight loss than usually advised limited-calories, low-fat diet + exercise. As an aside, ubiquitous assertion of harm from saturated fats is a huge fraud. An example of no-carb diet: fatty joghurt with neither sugar nor starch (fermented milk with nothing added), medium-boiled eggs, chicken or any meat, sour cream, fatty curd, plain water, orange juice without sugar added diluted in about 10 times with water, canned sardines, liver – eat as much as you want of these and when you want (not when clock tells you), but nothing else. No bread, no sweets, no salt, no spices/sauces. Take a vitamins+minerals supplement (like plain Centrum) all year round. Weight loss with no hunger, no exercise.
LikeLike
Hi Beverly, it’s really helpful that you write these articles. This is all far better than the majority of information on hrt out there and I hope others listen to you
I’m a 40 year old MTF with a background in bodybuilding and all that goes with that so I am a natural sceptic about doctors having all the answers to hormone protocols and their view of estrogen and testosterone .
I have always have had the view injections are by far the best most effective delivery method and the safest, for the liver etc.
I will be doing more research and if I do go on to use Hormones will definitely avoid Spiro and Fina, as I can’t see a good reason to use them….. Estrogen alone and maybe Progesterone make sense.
Thanks Alexa.
LikeLiked by 2 people
[…] via The Case Against Spironolactone — MTF Trans Hormonal Therapy […]
LikeLiked by 1 person
Both times I used spiro (both 9 month periods)it ends up in psychotic episodes and defeminization..I cant take this drug anymore so im currently in a estrogen only regimen.. Im so sad but the psychotic episodes were horrible and I wouldnt want to go through that.
LikeLiked by 1 person
Thanks for this article. I wish I saw this years ago spiro has destroyed my life. The list of sideffects are exhaustive. It masculinized me, my face, jaw, made hair grow on my body where it never was before, made my skin horrible, made my voice deeper, and gave me terrible mental problems, anxiety, depression, just to name a few, I was even prescribed meds for it that I wont take. Even my hair started thinning. I’ve been off it for about 3 months and still don’t feel like myself. Will I ever feel like myself again? I cry as I write this. I wouldn’t wish this on my worst enemy.
I started on estrogen first and felt unbelievable euphoria, after the spiro I was never the same. I did lots and lots of research and found out that spiro can actually activate androgen receptors wtf? Oposite of what we need. I also feel it increased dht which would account for the masculinization. I’ve never felt suicidal until I took the spiro. I never hated myself until the spiro. I was ok with every thing and was always relaxed now amost everything bothers me.
I want my motivation back. Is there any way to undo the damage that spiro has caused? And they wonder why the suicide rate is 40% amongst trans people. Screw aas. It saddens me even more to think that they’re still prescribing it to desperate girls. Any advice would be greatly appreciated. Bless n love
LikeLike
I was on Spiro for 2 years, at the end of it I ended up having surgeries delayed, due to the side effects not being known to my doctor. I was put through agonizingly painful tests on my muscles and nervous system, when Spiro was causing my symptoms. My legs and most muscles would just drop out at random and sometimes for up to 2 hours I couldn’t feel the ability to even flex a muscle in my lower body, it was typically just after anything that required me to stand still. When I ended up hospitalized because I was at that point losing the ability to walk or stand upwards of 6 hours a day, it was found the cause was intense dehydration, I was at that point drinking close to 3 gallons of water a day and because of spironolactone I had no ability to retain water. My doctors had me on several regimens prior to getting off of spironolactone, due to poor blood results. The month following my switch to finasteride, all of my levels were perfect.
LikeLike
Androcur (cyproterone acetate) causes depression, anxiety, fatigue or other mental disorders in 30% of MtFs. Finasteride in usually prescribed dosages (1-5 mg/day) can interfere with the progesterone->allopregnanolone conversion causing same side effects in some (fewer) MtFs, but finasteride dosage decrease to 0.05 – 0.1 mg/day (1/100 – 1/50 of a 5 mg pill once a day) prevents these side effects while giving equally strong useful effects (on hair only). There is a safe antiandrogen: bicalutamide 6-100 mg/day. But I agree, injectable estradiol valerate or cypionate at least 7 mg every 5 days without antiandrogen (with finasteride 0.05-0.1 mg/day in case of male pattern baldness in the past) is a safe and effective MtF HRT regimen. Moreover, it’s so safe for MtF and doesn’t interfere with any disease that no doctor checks, no blood tests are necessary. Of course, effects on libido, potency, fertility and social consequences of transition (or no transition with breasts) are your problems.
The most common disastrous thoughtlessness is taking hormones while postponing facial needle electrolysis.
LikeLiked by 2 people
Hello. Thank you for your input. Do you happen to know how it’s is interfering with progesterone>Allopregnanolone conversion? I’m guessing excess dht? Is that what causes depression? Thanks
LikeLike
Finasteride blocks 2 of 3 types of the 5alpha-reductase enzyme which performs both conversions testosterone->DHT in hair follicles and progesterone->allopregnanolone in the brain. Allopregnanolone is anti-depressive and anti-anxiety. Dutasteride blocks all 3 types and more often causes depression, so I don’t recommend dutasteride.
LikeLiked by 1 person
Is Cyproterone Interfering or sabotaging feminization in MTF too ?
I hope you can answer me, please
LikeLike
Cyproterone does not interfere with feminization like Spiro does, as far as we know, but since it is an antiandrogen it is associated with low-estradiol treatment regimens, which may be generally sub-par compared to estradiol-progesterone regimens.
LikeLike
So ultimately the best thing we can do is have an orchi or GCS as early as possible?
LikeLike
Or use an injectable estradiol ester (such as injectable estradiol valerate) at least 7 mg every 5 days. It’s safe and suppresses testosterone production by testicles without an antiandrogen.
LikeLiked by 1 person
The best alternative to using Spiro is to use Estradiol injections, or multiple patches, or implanted pellet, to achieve estradiol blood levels in the 350-700 pg/ml range, for at least a couple of years, which causes all testosterone production to cease in the body. No surgery is needed and this method is safe when done correctly, as proven by some studies. However, getting off Spiro if it has been used for years at megadoses (over 100mg a day) can require up to 6 months of a recovery period while your endocrine system rebalances. During that time false symptoms of testosterone may appear, even though testosterone remains low, because of the sensitized androgen receptors. However experience shows that patients taking megadoses can reduce to 100mg immediately without such problems, and then taper off slowly — as long as they are receiving estradiol as I mentioned above. Get your doctor’s approval.
LikeLike
I have heard that hrt involving spiro causes erectile dysfunction, infertility and testicular atrophy. I dont want any of those things,will you see any of those effects under an estradiol only or estradiol + progesterone routine?
LikeLike
Well I am 40 and presently on 200mg spiro a day and two 0.1mg patches of E for 6 or 7 months. Before that I was on 4mg oral E and 50mg of cyproterone for at least 18mths – it was definitely more effective but it ended up really screwing up my liver to the point of being admitted to hospital (AST/ALT >700). I can’t say I get brain fog or any of the bad symptoms suggested (at least anecdotally within myself without research). I am only pleased to be honest where I am at.
But forgive me for being analytical – I have a science degree – but the list of references doesn’t inspire me. A lot of the research is offline and 30 or 40 yrs old (I am looking offline soon), one reference is your own article (thats not a reference!) and one is an OUT magazine article (a good read tho). The one that does backup some of your claims (Leinung M) is a bit flawed as it’s measuring T levels but Spiro blocks T being effective and doesn’t actually stop production. The reference concludes correctly that it’s the E that drops production.
Do you have any other references? Happy to hear your thoughts.
LikeLiked by 1 person
The reference to my own article was linked to the statement “Studies at the time unfairly lumped all estrogens together, and all progestins together, as having the same dangers, a mistake which still lingers today.” which was NOT the main topic of the article and is intended to lead the reader into a branching path of knowledge. But I will edit the list of footnotes so it reads “References and Links” instead of just “References”. Oh, and I do have a science degree also. I didn’t expect to be graded on this one so it is done in a casual style. However I may be part of a formal paper later this year for WPATH. You can grade that one if you want. As far as the age of the references, the fundamental research on Spiro and some of the other points is of course very old. This is not a new drug by any means.
LikeLike
I continually upped my Spiro intake in an effort to aid feminization and facilitate a free path for E to do its thing. My E was 5 mg. every 7 days EC 5 mg. My results were dubious at best and I suffered many restless nights without sleep and the requisite muscle cramps spiro brings. I eventually added 5 mg. finasteride to this regimen per day to no avail. It neither changed my state of being, mind nor disposition as was proven out by my periodic bloodwork. Eventually, I chose to have SRS just to abate the perceived misery of the AA’s. The protruding belly, the lax and limp skin, the tired and broken feel and look, I was done. After the operation, I dropped the Spiro and Finasteride and increased my E protocol by double ( I presently take 40 mg. monthly in 3.5 day increments and enjoy perfect health at age 60 and have for nearly a year), I also finally received visual verification of feminizing via softer skin and actual fat redistribution,. I wish I had known how antithetical that anti-androgen therapy could be for trans women. Unfortunately, I was forced to discover the fact through my own trial and error. So much for transitioning in the stone age. Finding an Endo that will embrace this theology is nearly impossible.They are either to concerned with liability or to lazy to educate themselves.
Thank you, Beverly for your work and vigilance in effort to pave the way for women with our particular inbred handicap into the future. People like you, trailblazing for future generations are a true godsend. As an aside, I would like to include a member here named Lena Lenakiev, as well. She has opened my mind to my own possibilities and has enhanced my life immeasurably, Thank you Lena! One of you a political barn stormer and the other a patient alchemist with a heart. We need more people like you and are blessed to have you both in our presence during these trying times. Thanks you guys…you totally rock!
LikeLiked by 1 person
[…] are FDA approved for the purpose — and the resulting lack of trials and data means that patients themselves often provide the expertise, and must bear the burden of being the sole experts on their own bodies and often on their care […]
LikeLike
I feel really bad for asking this, but Im a cis woman on spiro for acne/pcos issues. Ive noticed a difficulty in loosing weight since starting it, and I also have had a hump in my neck thats grown significantly since I started the 200mg dose I’m on. Could an increase in cortisol be to blame for this in me as well?
I understand you can’t make conclusive statements without seeing specific data, of course. I’m just curious.
LikeLike
You can take bicalutamide 50 mg pill every 1-3 days instead of spironolactone.
LikeLike
the hump on your neck can definitely be from raised cortisol levels. Cushing syndrom can be causes by medication like this.
LikeLike
[…] via The Case Against Spironolactone […]
LikeLike
Hi, thanks for reading.
Im a 32 years old man, and I need some help to reach my objective. I will look for an endo, but before doing this, i need some info.
I cant start my transition before reaching 40, but, right now, I want my body to be sweet as I am inside.
Basically, I want some breast development, around b cup, and some more fat in the butt and hips. Its something important to me…
I dont want to lose my libido, but I dont matter about erections.
Do you think a combination of oral estradiol with gel, like Sandrena, can work?
If I decide, later, to stop, I will keep some breast, maybe regreting to A cup. And what about the fat stored in butt and hips? What happens?
Sorry for my low quality english, and thanks for tour attention!
LikeLike
What if u have been on spironolactone 200 mg for 10 + years? Can u still go off of it?
LikeLike
[…] de “The Case Against Spironolactone”, texte de Beverly Cosgrove, 22 Décembre 2018, Version […]
LikeLike
I used spironolactone for about a year and am luckily off it now but it helped with a colonoscopy. I was wondering if there is a hormone that increases your breast size but leaves your testicle activity alone?
LikeLike
I was a sex worker at one point in my life and didn’t need hormone replacement therapy.
LikeLike
Are you a doctor?
This is all selective and anecdotal at best.
LikeLike
you’re feeling attacked because you’re on spiro and you are threatened
don’t defend spiro.
LikeLike
The references and research are not “anecdotal”. Do the reading and research yourself, if you wish.
LikeLike
It’s now July 2019, and online pharmacies are still (from late 2017) claiming that injectable estradiol is still “not manufactured & supplied”. Nor do they know if or when things will improve.
Is this a conspiracy ? – Or ‘Sales’ mismanagement???
I used to use the brand Progynon Depot 10mg/1ml and inject two vials per week. No spiro…and my T levels were measured after 9 months and were on the lower end of the Female range.
My breast growth was acceptable – nearly C cup – and best of all, male pattern baldness ceased and one barber claimed to see re-growth…
Any ideas on supply ? I miss that wonderful feeling of inner peace, – both mental and emotional – and the more considerate person I used to be ! 🙂
LikeLike
That was exactly my experience. I had started on sublinguals but felt a need to enhance their effect. I was instructed to take one vial a month, but after a few months it didn’t feel adequate It wasn’t until I was injecting 8-10 vials a month that I was enveloped by the “wonderful feeling of inner peace”. It didn’t feel the least bit excessive; there was just a sense that my thoughts and emotions radiated from a feminine core. And I too was a much more calm and considerate person.
Most of us have lived for decades with a testosterone enriched body. To believe that a HRT dosage designed for a woman will satisfy our transitional needs is head-in-the-sand inanity. I want that beatific calm back.
LikeLike
[…] plus prescrits sont donc la spironolactone (un diurétique ayant par ailleurs écopé d’un récent remontage de bretelles en règles) et le bicalutamide, l’anti-androgène présentant comparativement le moins de risques pour […]
LikeLike
Wow thanks for al this information. I’m mtf 34 and willing to start HRT next month.
I was gadering studies about the effectiveness of different prescriptions for hrt.
I would like to ask if I’m correct in the order of effectiveness/fewer side effects, from better to worst in the following A blocker list:
1- b17 estradiol only
2- GNRH antagonists
3- Bicalutamine
4- Cyproterone
5- Spiro
LikeLike
38 transwoman. Vegan diet. No alcohol use. Started HRT in August 2016. After approx 3 years of Estradiol at 2mg, 2x per day & Spiro at:
Initial dose 100mg, 2x per day – experienced dehydration, extreme salt cravings, increased anxiety, brain fog, and narcolepsy (as a result of frequent urination throughout the night).
Increased dose in Oct 2018 to 150mg, 2x per day – same symptoms as mentioned previously and additional symptoms of short term memory loss & dry eyes.
Increased dose in July 2019 to 200mg, 2x per day – same symptoms as mentioned in previous 2 dosages except much worse. Additional symptoms of crippling leg and foot muscle cramps. I took the dosage for about 2 weeks and lowered dosage back down to 150mg 2x per day without much relief from new heightened symptoms. The dehydration was the worst.
Oct 2019 – After talking with dr a out symptoms, she changed hormone regime to .3mil of injectible estrogen valerate 1x per week without any anti androgen. It has only been 1 week, but the side effects from spiro are slowly disappearing. Giving myself a shot in the stomach is a little scary, but it isnt nearly as bad as the suffering I endured from spiro. I’ll write an update once I am further along with my new prescription.
Thanks for the info on this site – it helped me decide which new hrt option my doctor offered would be best for me.
Peace and love to my sisters.
LikeLike
I’ve taken oral estradiol 2mg/daily and 200mg/day spiro for a few months now and things have been going okay thus far but every time I start to see information like this I am filled with immense anxiety about my transition. I live in the US and am fairly limited financially at the moment. I’m at a loss as to what I should do here, should I raise these concerns to my endo at the next appointment (in about 6 weeks)? The only real side effects from it I have suffered is a bit of the fogginess which comes and goes. What would be a better option for me? I can provide further details as needed.
LikeLike
You are on the “orthodox protocol” from the 1990’s, like many. If you read the articles elsewhere on this site, you’ll see that in most cases the best option is injection of estradiol valerate or other estradiol ester once a week or more often, by subcutaneous or IM, and no antiandrogen is required normally with that regimen.
LikeLiked by 1 person
In your opinion is it safe to stay on my current regimen through the holidays until I see said doctor again or would it be wise to try to discuss these concerns with my endocrinologist like, now. I don’t think I’m meant to stay on this current combination for long as I only started estrogen in August.
LikeLike
What do you do if you just can’t stand needles….
LikeLike
I can’t advise you individually, but in cases where a patient is taking Spiro megadoses, the literature implies that the dose can be immediately reduced to 100mg a day without severe side effects, but from there, one should reduce slowly over a period of days or weeks — but you should not make changes without contacting your doctor. Also, be warned, that endocrinologists are usually unaware of these issues.
LikeLike
thank you so much for this info. it saved me from jumping on the spiro wagon which would have caused me unwanted problems. im sure im not the only one you’ve helped. sharing this info, which is not available on clinic websites that are practicing the spiro + e approach is priceless to people like me who are new to transitioning. i really cant thank you enough. im on e only and i plan to switch to injecting based on your other post on subcut injections.
LikeLike
I’m taking 75mg of spiro and 2mg of estradiol a day to cut down would I drop 25mg and take 50mg for a while then drop it to 25mg then then nothing ? when I went to my 6 mth checkup my t level was like 178 and estrogen level dropped to 33 but last time when taking 25 mg of sprio my estrogen level was higher at 50 at my 3 mth checkup was it the spiro that lowered the estrogen level then ?
LikeLike
[…] that all trans women who are considering taking it, or taking it, read this article – The Case Against Spironolactone. Furthermore, following the Dr. Will Powers method of transition, I found that I did even need it. […]
LikeLike
I got off of it after two months and I thought one night I was going to have a heart attack. It’s awful stuff. I was having a bad skin reaction to estridol patches. So I was glad to get that out of my system. I’ve been hearing a lot of great things about Bicalutamide recently. One of my trans girlfriends highly suggested it. I think someone listed it above taking it once every three days. I would love to hear the feedback from anyone who’s been on it?
LikeLike
I’m 25 and on 400mg a day, everything’s been going fine for me. Not as much breast growth / gyno as I wanted but over all things are peachy keen otherwise, bit more peeing is all.
LikeLike
I wonder if I might have that oft-bandied about pseudocondition of adrenal fatigue, because the moment I took spiro at the same time as frankly underdosed patch estradiol, it was like I was a new woman – bursting at the seams with confidence, motivation, and energy, attracted to and mindful of my own appearance (even though it had not changed one whit), typing style changed, total depression remission.
LikeLike
My experience has not been typical of what you have described here. I have been on a megadose of spiro for about 20 months now. I am under the care of an endocrinologist at Duke in Durham, N.C. I am 52. My baseline bloodwork, which was done before I began an HRT regimen showed very low levels of testosterone (100) and an estrogen level of 25 which was pretty shocking to me. I started out on 100 mg of spironolactone which dropped my T levels down to half of what they were according to the blood work that was done 3 months later. The dose was increased to 200 mg around which time I noticed a marked drop in erectile function, followed about a month later by a complete absence of ejaculation. Later blood work showed my testosterone “nicely suppressed” in the words of my endocrinologist. During the following year, I have noticed very significant genital shrinkage. Wearing a gaff is almost unnecessary now, a little more shrinkage will get me there. I am really wondering if I could just taper off the spiro (under the guidance of my Dr.). My testicles are the size of peanuts now and are somewhat difficult to even find, even though I have experienced significant scrotal shrinkage as well. I have read elsewhere in my research that the body’s ability to produce testosterone is eventually permanently damaged or destroyed. If that is the case, I think that it won’t be much longer until I reach that point considering the physical changes to my genitalia and the weekly delestrogen injections will be sufficient to complete my transition.
LikeLike
Your initial levels of Testosterone were already within the female range before you began HRT, so clearly Spiro was not responsible for lowering your T. You did not mention what estradiol you are taking, and I’m assuming that your HRT is not a Spiro-only one, so it is almost certain that the drop in T that followed was due to beginning the estradiol and was not related to the Spiro. Treatment with an antiandrogen only is not generally considered a feminizing regimen because a male hormone balance does not become a female hormone balance simply by removing Testosterone from the patient. Likewise, suppression of ALL sex hormones, as with a GNRH agonist, without adding sufficient estradiol, is not feminizing either.
LikeLike
I have a gene mutation that makes me feel Estrogen is too risky. My doctor put me on Spiro, very low dose but I got dizzyness, headache, extreme fatigue, tired, heavy legs, exhausted. I could hardly skateboard and do yoga. It was like I had 40+ C fever, but no fever.
First I thought it was pollen allergy. 4 days off Spironolactone I feel better.
Now I don’t know what to do. I am afraid of medicine and was proud I dared take Spiro. What about Orchiectomy? Can that be an option? I have read some transgender opt for that.
I also take Femarelle, but have no idea it does anything … but my doctor suggested I tried it.
LikeLike
I’ve so far not had any issues with spiro. I started HRT in March of this year, so I’m at 6 months. I’ve been losing weight, I’ve not had any brain fog or dizziness, or anything. At 200mg a day, I’ve found that my body hair is growing much slower than before. My estradiol levels are at 151 pg/mL, and I’m taking just taking 6mg of it orally a day. I’m getting my t-levels checked in 6 months (for the first time, since my endo never checked it before) and we’ll see if t is being suppressed properly. If not, I’ll start progesterone. (Endo also says that there are no studies that say progesterone helps with anything other than suppressing T further? I’m not sure about that one, though…)
LikeLike
[…] are based on unreliable research – but I have to start somewhere. I was also suffering from 7 of the most common side effects of the anti-androgen drug my doctor had prescribed, spironolactone. (Not counting the listed side […]
LikeLike
Hi, I’m 22 now I’ve been on spiro since I was 16. I’m just now finding this out and I feel as if my endocrinologist has fucked me. I am kind of freaking out.
If I get on another T blocker will I be able to achieve the feminizing effects I would have had, had I not been on spiro for 5 years? I’m worried now that I will not be able to pass as well now as I could have and even if I were to stop all it would do would prevent further damage rather than reversing it…
Thank you for writing about this.
LikeLike
[…] So while we’re on the topic of HRT, I also did some reading and thinking at the hotel about that. For one thing I found an article by Alex V. Green about spironolactone use on Slate titled “Spironolactone, a Standard Drug in Hormone Treatment for Trans Women, Has Controversial Side Effects,” and it also links to a source article by Beverly Cosgrove called “The Cast Against Spironolactone.” […]
LikeLike
[…] recommend that all trans women who are considering taking it, or taking it, read this article – The Case Against Spironolactone. Furthermore, following the Dr. Will Powers method of transition, I found that I didn’t even need […]
LikeLike
I would love to have a more “feminine” figure, which includes breast growth and increase in size of hips and butt. However, I’ve decided against hrt because I don’t suffer genital dysphoria and i have no desire for my genitals to shrink or lose erectile function. My question is, if i were to take estradiol only, patches, would my genitals still atrophy and become useless as far as sex is concerned? Or would my genitals retain their present size and function? A related question regards my age. I’m 62, tall and slender except for a small bulging belly. Will my age be a cause of reduced breast growth, or is breast growth strictly dependent on genetics? Thanks!
LikeLike
The answer to your question is quite complicated and you will probably have follow up questions, so I suggest joining the MTF HRT Hormone Forum on facebook, which I run, and make a post there to get a detailed answer.
LikeLiked by 1 person
Your age shouldn’t be an issue for reduced breast growth as far as I can tell, I wouldn’t worry about that. And in my experience using estradiol patches, you won’t get an erection quite as easily but you still should be able to. This is all personal/anecdotal evidence so take it with a grain of salt, but that’s my two cents.
LikeLiked by 1 person
[…] messes with renal function and potassium metabolism, I expect that it affects this. Digression: spironolactone is total bullshit as an anti-androgen of first resort. It sucks and I hate it and I should have switched to other […]
LikeLike